

A Note on Peptides
Novo Nordisk, Eli Lilly, Hims & Hers. Everyone is betting on peptides. We've been quietly trying to figure them out for a year. Here's an update on peptides as a supplement brand.

👋🏼 Hi, I’m Shan. I run Xandro Lab, a longevity science brand in Singapore. Every Sunday I write these notes. They are part building diary, part thinking out loud. Sometimes, it is marketing or operations. This week it’s about something I’ve been wrestling with for over a year - peptides (read Ozempic, BPC-157).
")
Peptides are all over my feed right now. And they’ve been in my head even longer. At Xandro, we’ve been quietly evaluating one specific peptide, BPC-157, for last few months. I haven’t talked about it publicly until now, because we still haven’t figured out whether we can bring it to market in a form that actually works.
That’s the story I want to tell today. But before I get to our journey, let me explain what peptides actually are - the science here is genuinely interesting, and also genuinely complicated.
(insider note - the scientist was blown away reading the results from peptides)
In this issue:
What peptides actually are
The ones worth knowing: GLP-1, BPC-157, GHK-Cu, Retatrutide and others
A 100-year-old unsolved problem: why oral delivery is so hard
The grey market flooding in from China and what HSA and FDA are saying
The Hims & Hers episode: what happened when the company skipped the science
Where we are at Xandro with BPC-157
1. So what even is a peptide?
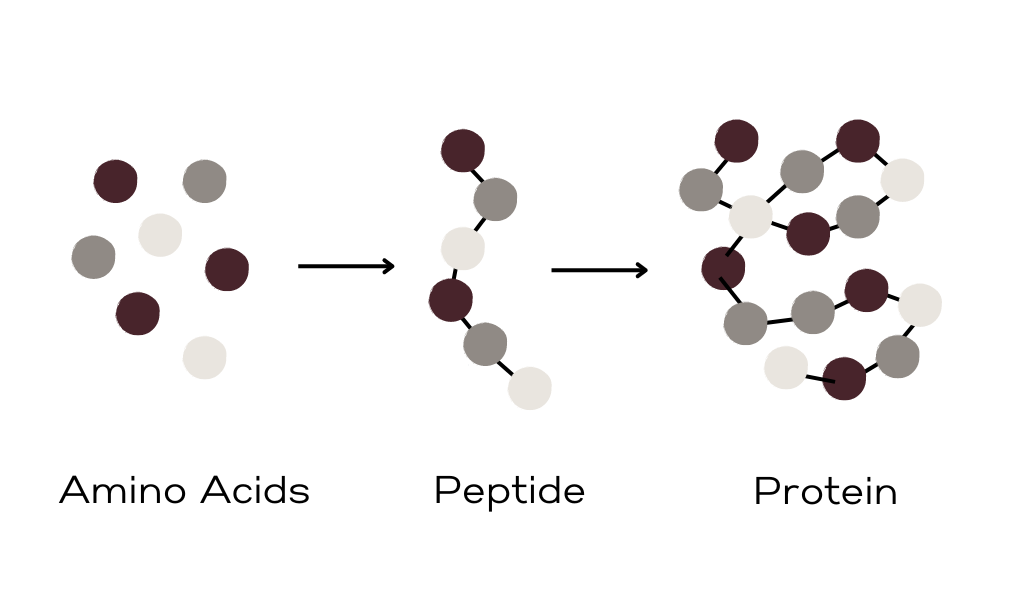
Proteins are long chains of amino acids, sometimes hundreds of them linked together. Peptides are just shorter versions of the same thing. Our body produces them naturally. They act as signals - telling your cells to repair tissue, regulate hormones, manage inflammation, control hunger. They are molecular messengers.
The reason people are excited about synthetic peptides is this: what if you could take a specific messenger your body already uses and give yourself more of it? What if you could send a louder signal for tissue repair, or for fat burning, or for gut healing?
That’s the promise. And the early research is genuinely exciting.
Isn’t this just like collagen peptides?
I get this question a lot, especially from people who train. It’s a fair one, because the word “peptide” gets used for everything from gym supplements to grey-market injectables, which creates a lot of confusion.
Collagen peptides and dipeptides — the kind you find in protein powders, collagen drinks, and recovery supplements — are short, simple 2-3 amino acid chains. They’re food-derived, structurally straightforward, and your gut has specific transporter machinery designed to absorb them efficiently. They work as building blocks, providing raw materials your body uses to rebuild tissue.
The therapeutic peptides we’re talking about today are a completely different category. They’re longer, structurally complex molecules engineered to bind to specific receptors and trigger very precise biological responses. Think of a dipeptide like a two-word text message — easy to read, hard to misinterpret. A therapeutic peptide is more like a legal contract. Every word and punctuation mark matters. Destroy one clause and the whole document is useless.
This distinction matters a lot, because it’s the reason that what works fine in a collagen drink becomes genuinely unsolvable in a therapeutic peptide context. The gut that easily absorbs a collagen dipeptide will systematically destroy a BPC-157 molecule before it can do anything.
2. The peptides getting the most attention right now
GLP-1 agonists like semaglutide (Ozempic, Wegovy) mimic a gut hormone that regulates appetite and blood sugar. The weight loss results from clinical trials were unlike anything the industry had seen before. They are already reshaping how the world thinks about obesity and metabolic health.
Tirzepatide (Mounjaro, Zepbound, Eli Lilly) is a dual agonist — it hits two hormone receptors, GLP-1 and GIP. Stronger results than semaglutide. Already approved and widely prescribed.
Retatrutide is where the pipeline gets genuinely remarkable. Still in Phase 3 trials, but the data from Eli Lilly is staggering — up to 28.7% body weight reduction in 68 weeks. It’s a triple agonist, activating GLP-1, GIP, and glucagon receptors simultaneously. Analysts forecast FDA approval around 2027. The pharmaceutical industry keeps escalating — from one receptor to two to three — and the results keep climbing with each generation.
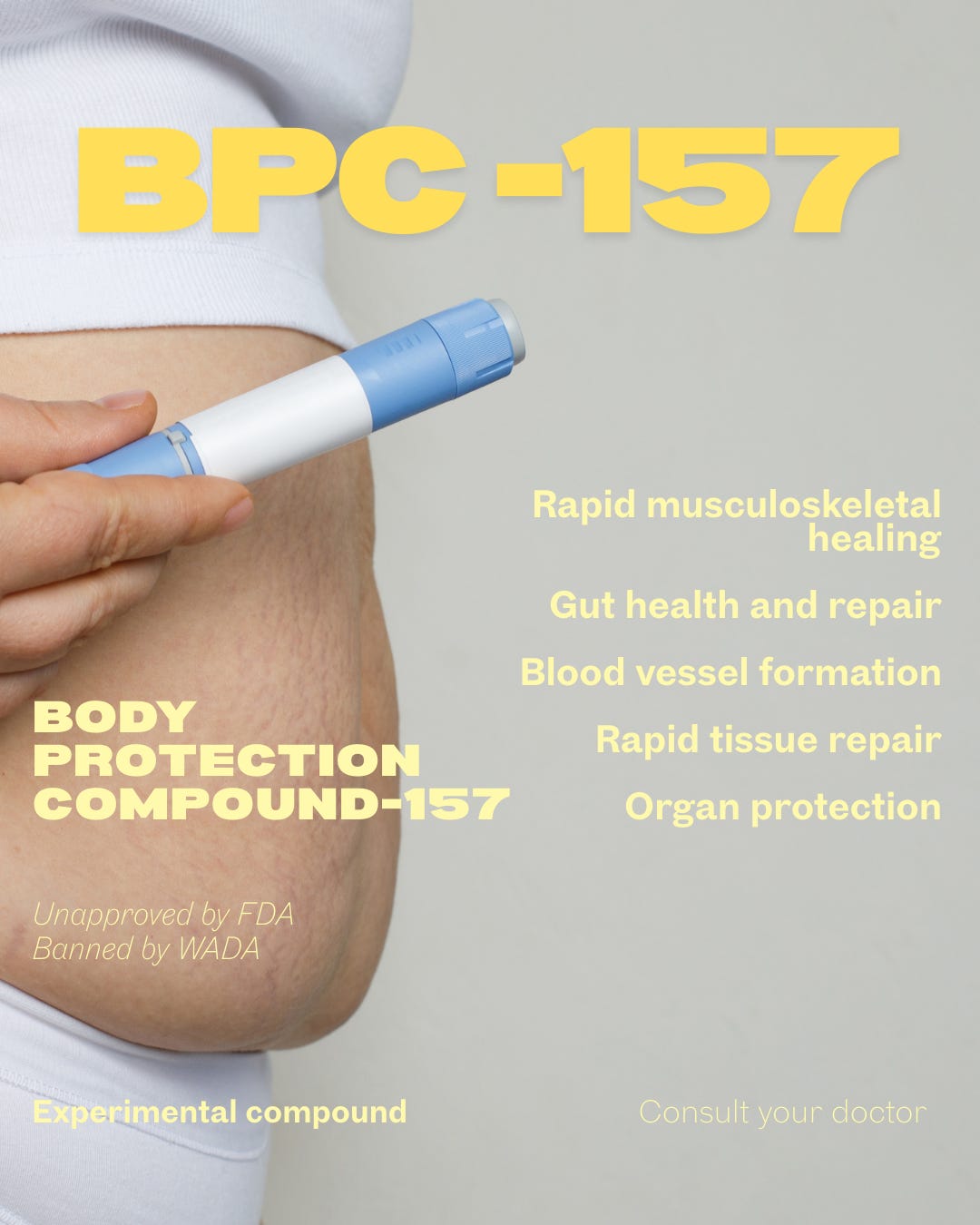
BPC-157 (Body Protection Compound 157) is a peptide derived from a protein found in human gastric juice. Animal studies show accelerated wound healing, tendon recovery, gut repair, and neuroprotective effects. For someone in their 40s or 50s dealing with chronic inflammation or an injury that won’t resolve, the promise is obvious. The challenge is that almost all the research is in rodents. Human trials are sparse.
TB-500 is a synthetic version of thymosin beta-4, involved in tissue repair and regeneration. Similar profile to BPC-157 in terms of the excitement and the evidence gaps.
GHK-Cu and AHK-Cu are copper-binding peptides that your body naturally produces. Their levels decline significantly with age. GHK-Cu drops from around 200 ng/ml in your 20s to about 80 ng/ml by age 60, and that decline tracks closely with the body’s decreasing ability to regenerate tissue. Research shows GHK-Cu stimulates collagen and elastin production, supports wound healing, and has anti-inflammatory effects — which is why it already appears in high-end skincare. AHK-Cu works through similar copper-binding mechanisms with a focus on scalp and hair follicle health. Both are interesting from a longevity standpoint specifically because they’re not foreign compounds — they’re things your body made abundantly when you were younger. The research here is more developed than BPC-157, particularly for topical delivery, though systemic delivery remains an open question.
The overarching idea connecting all of these: the goal isn’t to introduce something foreign. It’s to amplify processes your body already runs — just louder, and for longer.
3. A 100-year-old unsolved problem
Here’s the fundamental challenge that doesn’t get enough airtime in the peptide conversation.
Your gut is essentially a 30-foot disassembly line for proteins. Stomach acid, digestive enzymes, the mucus layer in your intestines — the whole system’s job is to break down anything that looks like a chain of amino acids into its component fragments. Collagen dipeptides were designed by nature to be absorbed this way. Therapeutic peptides were not.
Sean Geiger wrote a sharp breakdown of this history that’s worth reading in full. The numbers are sobering. The first attempt at oral insulin was in 1922, one year after insulin’s discovery. Since then, 13 different companies have tried to crack oral insulin delivery. Not a single commercial product exists after a century of trying. Peptide drugs on average have oral bioavailability below 1-2%. For comparison, metformin — one of the most common diabetes drugs in the world — has bioavailability of 40-60%.
So when Novo Nordisk announced an oral semaglutide pill, it was a genuinely remarkable scientific achievement. They did it using a molecule called SNAC — a permeation enhancer that took decades to develop, required a $1.8 billion acquisition of the company that created it, and involved over 9,500 patients across ten Phase 3 trials.
The result? 0.8% bioavailability. Meaning 99.2% of what you swallow is still destroyed. That 0.8% is the entire product. And SNAC is so molecularly specific to semaglutide that when Novo tried it with liraglutide — a closely related GLP-1 drug that differs by a handful of amino acids — it didn’t transfer. The technology doesn’t generalise.
Why does it matter that the stomach breaks them down?
This is the question I kept sitting with. Here’s the answer.
When your body produces a peptide naturally, it doesn’t send it through the digestive system to reach its target. It produces it locally — right at the site where it’s needed — or releases it directly into the bloodstream from cells or glands. The stomach acids are never in the loop. GHK-Cu is cleaved from proteins in the extracellular matrix right at the site of tissue injury. BPC-157 is present in gastric juice as part of the gut’s own protective system — it doesn’t need to travel anywhere to do its job.
When you take a therapeutic peptide orally as a supplement, you’re asking it to survive a process it was never designed to go through. The amino acids might still be absorbed — but the specific sequence that makes the molecule biologically active is gone. It’s like shredding a contract and then absorbing the paper. The material gets in. The message doesn’t.
This is why research settings default to injectables — bypassing the digestive system so the compound reaches circulation intact. But that creates its own problems for consumer use: sterility, dosing accuracy, refrigeration, and the simple reality that most people are not going to inject themselves every day.
4. The grey market problem
Here’s what access actually looks like right now.
I get multiple messages a week from peptide suppliers, most of them based in China. Injectable BPC-157, TB-500, and GLP-1 analogues are being shipped directly to home addresses across the world with essentially zero friction. No prescription. No clinic. Just a credit card and an address.
Singapore’s HSA has issued warnings about this. The FDA in the US has too. Both specifically flagged the risks of using injectable peptides without medical supervision and much of what’s circulating has no quality verification at all. You genuinely don’t know what’s in the vial. Contaminated batches, incorrect concentrations, unsterile preparation. And that’s before asking whether the compound is even what the label says it is.
I understand why people do it anyway. The promise is “promising”. The wait for proper clinical validation is measured in years, sometimes decades. For someone dealing with a chronic injury or a condition that conventional approaches haven’t fixed, years feel like a long time. I get it. But the risk profile is real.
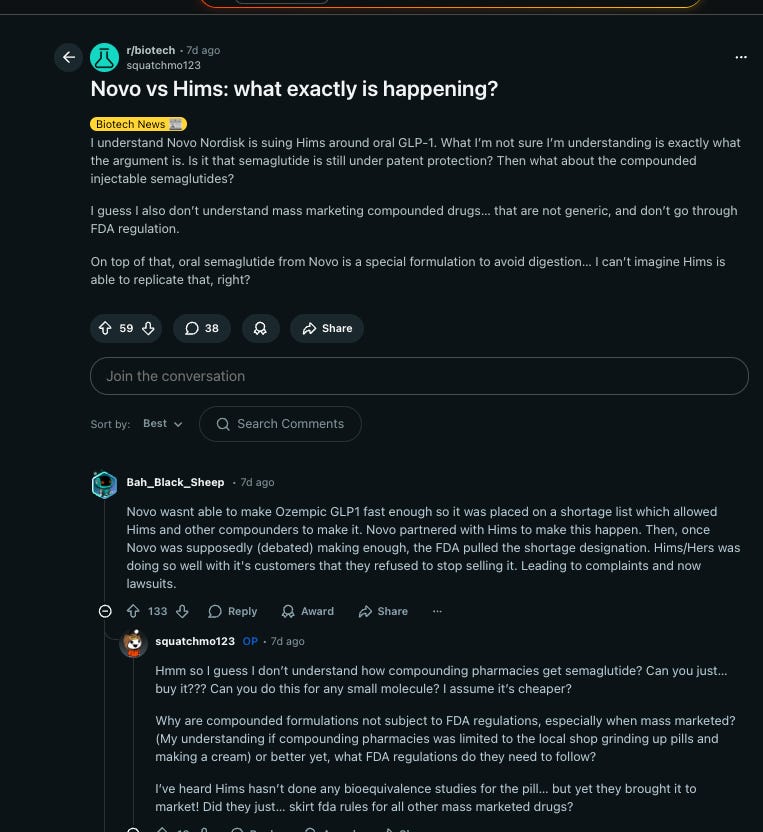
5. The Hims & Hers episode
The most instructive case study in this space played out almost entirely this month.
Hims & Hers had been selling compounded injectable semaglutide since 2024, positioning it as an affordable alternative to branded GLP-1 drugs during a supply shortage. Then in early February 2026, they announced a compounded oral semaglutide pill at $49 per month versus Novo Nordisk’s $149.
Within days: Novo Nordisk filed a lawsuit. The FDA announced action to restrict the active pharmaceutical ingredients being used in knockoff products. Hims pulled the pill almost immediately.
But the deeper criticism was scientific. When Reuters asked Hims what absorption technology their oral pill uses, the company said “liposomal technology” and declined to elaborate. No published pharmacokinetic data. No bioavailability studies. No human clinical trials. As Geiger notes — Novo spent decades and over a billion dollars developing SNAC, and still only achieved 0.8% bioavailability. Hims had none of that.
The FDA referred the case to the DOJ. Hims’ stock dropped over 60% from its highs. And the regulatory grey space of 2024 had by early 2026 narrowed into something much less forgiving.
6. What we found when we looked at BPC-157
Over the past few months, our team has been evaluating BPC-157 as an oral compound. We focused on it because it’s considered one of the more stable peptides in this class (a more realistic candidate for oral delivery). We cannot do injectibles since that falls under the medicine purview.
Challenge is - “More stable than other peptides” is not the same as “stable enough to work.” What we have found was discouraging: in standard oral delivery formats, BPC-157 may degrade before it reaches systemic circulation in a meaningful concentration. Not harmful. Just potentially useless.
I am not willing to put a product on a shelf and charge people for something that’s probably useless. That’s dishonest at best, and it takes money from someone genuinely trying to improve their health and gives them nothing in return.
So we haven’t launched. But I haven’t given up either.
We’re currently exploring whether specific encapsulation technologies could protect BPC-157 through the digestive process and allow for effective oral delivery. It’s a genuine open question. If you are someone working in this field, and would like to speak more, drop me a note at shantanu@xandrolab.com.
The tension of building in longevity and health
There’s a version of this story where I just announce a BPC-157 product and ride the wave of interest that’s clearly building. People are asking about it. Competitors are preparing launches. The commercial pressure is real, and I feel it.
But here’s what I keep coming back to. We’re not Unilever. A company like that can make mistakes and still be fine five years later because of scale. We don’t have that cushion. In this industry, a brand can die with a few bad months — from a product that doesn’t work, from regulatory action, from a reputation hit with the audience.
So we wait. We work. And when we have something worth putting in front of people, I’ll write about that too.
Closing note
Peptides are not a fad. The biology is real, the pharmaceutical investment is enormous, and the pipeline keeps escalating — from GLP-1, to dual agonists, to triple agonists like retatrutide, with each generation producing results that would have seemed impossible a decade ago.
For the supplement world, the question isn’t whether peptides will matter. It’s whether we can get delivery right — oral, accessible, effective — without cutting corners on the science.
We’re still working on the answer.
Cheers
Shan
The science section of this post was informed by Sean Geiger’s excellent piece A Brief History of Oral Peptides — strongly recommended if you want to go deeper on oral delivery.
Additional note - peptides also present a huge regulatory hurdle for dietary supplements companies. They are regulated like medicines. However, oral forms are somewhat in grey area like BPC-157. Xandro operates in the non-regulated dietary supplements space as of now. So we will need to tread carefully. In future, we do wish to move towards the regulated space with required licenses. It’s a few years away though.